If you use a closed-loop insulin administration system (Medtronic 770G and 780G, t:slim with Tandem Control-IQ), also known as an automated insulin delivery system (AID) or commercial artificial pancreas, you know that you need to calculate the carb content of your meal and enter it manually into your pump before eating.
And if you don’t enter all the carbs you eat, will the system be able to compensate like it does when your blood sugar is trending up? That’s what a group of scientists from Israeli universities and US company Medtronic sought to find out.
To achieve this, the scientists compared the ability of the MiniMed 780G pump to understand and correct rising blood sugar levels when meals were “announced” by users and when they weren’t. They found that it’s best to always enter your carb counts into your pump, especially if your meal is high in carbs. In the case of low-carb diets, it seems that the system is able to compensate and limit the increase in blood sugar.
Unannounced meals: not dangerous, but not recommended either
Commercial artificial pancreases work based on an algorithm (a series of calculations in the form of software) that automatically manages insulin administration based on the real-time blood sugar readings received from a continuous glucose monitoring system. Using this data, the algorithm can correct hyperglycemia by automatically administering a correction bolus.
However, it’s important to remember that these systems are not completely self-sufficient. You need to manually enter into the pump the number of carbs you’re going to eat, so that the algorithm can calculate the required bolus for your meal. If you omit or forget to announce your meal to your pump, there’s an obvious risk of significant hyperglycemia because you won’t receive the required insulin dose beforehand.
This task can be difficult for some people for different reasons, including the need to calculate accurately, to anticipate activities, etc. That’s why researchers from around the world are conducting different projects to find a simplified carb counting method.
With that in mind, the Israel-US study followed 14 participants with type 1 diabetes (T1D). The scientists first tested two approaches, i.e., entering or not entering carb counts into the pump, in a secure environment for five days. After that, participants returned home and were instructed not to announce meals with 80 g of carbs or less to their pump for a total of 90 days. Then, for 90 further days, participants were instructed to announce the carb counts of all their meals.
The purpose was to assess whether it was safe for participants’ health not to enter all the carbs they ate into the pump.
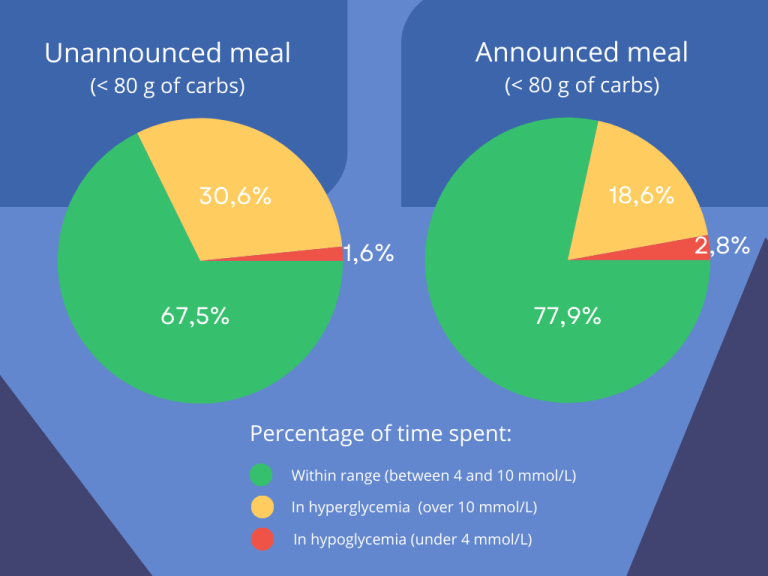
The study found that participants spent more time in hyperglycemia (over 10 mmol/L) and less time within target blood sugar levels (between 4 and 10 mmol/L) in the period when meals with 80 g of carbs or less were not covered by pre-meal insulin doses. However, they spent less time in hypoglycemia.